

Our world has been transformed by data. As we transition into data-driven societies, it dictates what we see online, how we live our lives, and what food we buy. Governments also use data to understand how to tackle challenges, using ‘data-driven policy’ to react to societal questions on migration, poverty, and climate change.
It is therefore hardly surprising the important role data plays when we find ourselves in the midst of a crisis, and how people seek assurance in data, before they do their own governments. This paper explores how data-driven policy making can teach us a threefold approach for using data in a pandemic in the immediate, near, and long-term.
It can tell us how governments should react
Data can help governments, but only if governments seek to collect data. That is why governments with the available resource have been using testing as a means to gain data on it’s citizens to enable policy making. By widespread testing, governments can gain a better understanding of not only the scale of the problem, but specific areas and the patterns in how it is being spread (through human behaviours).
Governments test citizens for two main purposes. Firstly, for the individual to know whether they have contracted Coronavirus, and therefore, need to be quarantined (this is particularly important for key workers who may be more likely to pass the virus on). Secondly, to work how far it has spread to inform decisions around social distancing and lockdowns.
You only have to look at the countries that have implemented widespread testing to see clearly, that they have been the most effective in curtailing the virus, including Germany and South Korea.
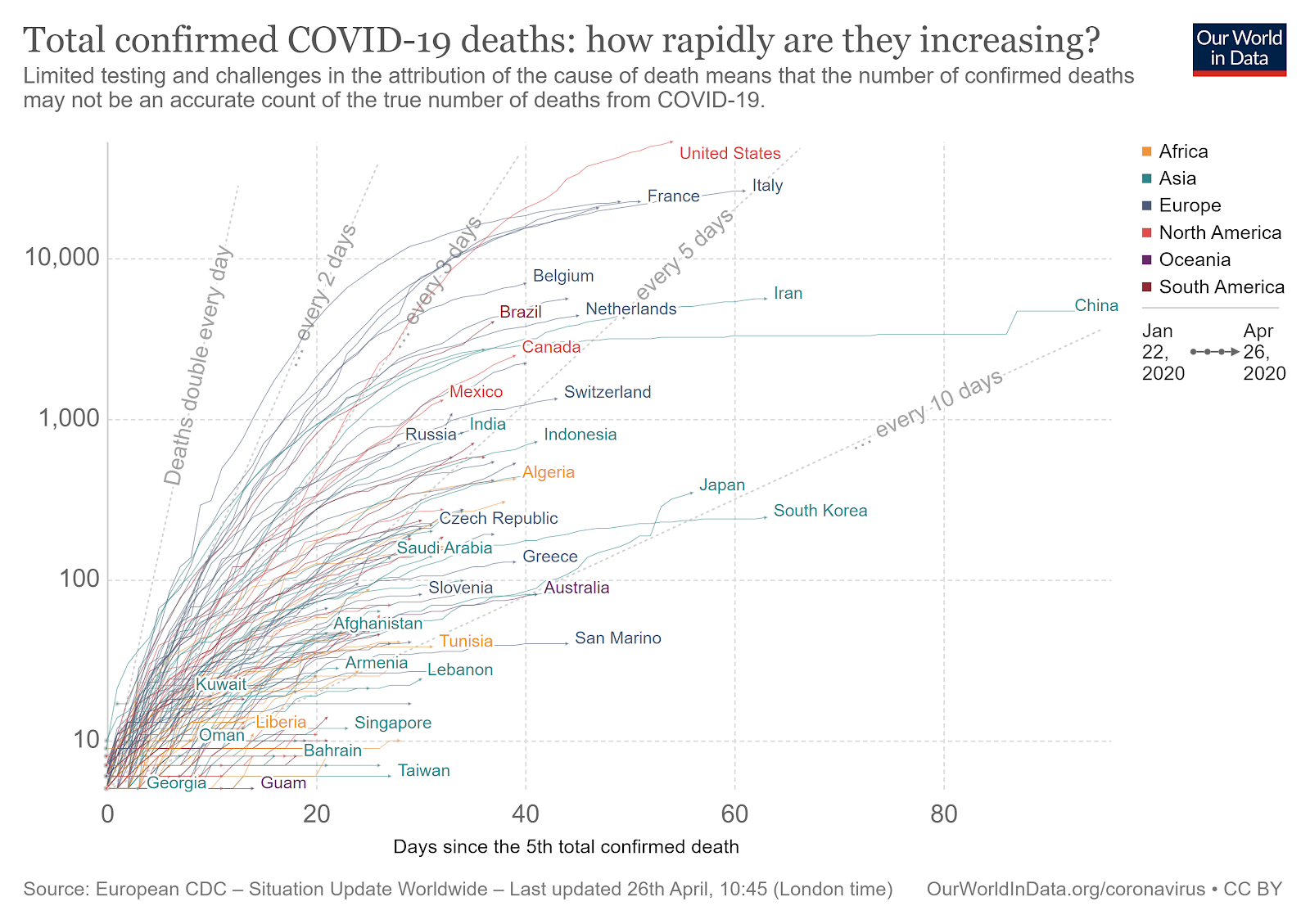
South Korea and Germany, with widespread testing and early lockdown, flattened the ‘curve’ whilst other countries struggled to control the outbreak. Source: Our World in Data
Those who have not had the resources available, such as developing countries, or only realised too late the important role testing would play, have been looking to other means to gather data. Most notably, by using mobile apps to allow governments to track whether citizens have symptoms and who they have been in recent contact with.
Last week, more than a million Australians downloaded a coronavirus contact tracing app within hours of it being released by the government. The COVIDSafe smartphone app uses a Bluetooth wireless signal to exchange a “digital handshake” with another user when they come within 1.5m (4.9ft). The app then logs this contact and encrypts it.
Users will be notified if they have had more than 15 minutes of close contact with another user who tests positive. Although Australia has a considerably lower death toll than other countries, the government is hoping that the data gained from the app will allow them to determine whether they can ease lockdown restrictions. Countries, such as Singapore and the UK, have already been using app data.
It is important for governments to make informed decisions, particularly when lives are at risk. Using data, preferably through a formal diagnosis, but occasionally through self-diagnosis, allows governments to make these important decisions around lockdowns, civil liberties, and resourcing. Otherwise, they may as well be drawing a line in the sand.
It can tell us how health systems should respond
As COVID-19 started to take hold of Europe, governments were keen to reassure citizens that there were clear people who were at risk. These categories include the over-seventies, those with underlying health problems, and those who smoked.
But these situations are fluid and often, data can throw out unexpected results. Health systems need to respond to these emerging trends.
In the UK, the more we learnt about those who were dying, the more we started to suspect that the categories of those who are at risk were more nuanced than previously thought. The faces of doctors who had unfortunately died because of Coronavirus seemed to have something in common: they were overwhelmingly BAME. In fact, the first 10 doctors in the UK named as having died from the virus were all BAME.
Ethnicity frequently plays a role in health disparity, as certain groups may be more ‘at risk’ than others. In the UK, black women are five times more likely to die in childbirth than white women and some BAME groups are more likely to develop mental health problems. Health disparity is often not the result of genetics, but down to socio-cultural influences, such as language, income inequality, or unconscious biases that leads others to viewing the symptoms of a BAME person as somehow less legitimate.
It is therefore not only important to gather comprehensive data on those who are dying or have contracted the virus. With patients from ethnic minority backgrounds over-represented in critical care units and among healthcare staff who have died, it is clear that failure to explore this data can put lives at risk.
Real-time data collection, layered with anecdotal research, can really help health systems in understanding which patients are more at risk and how to safeguard against further fatalities in the immediate future. It is equally important for countries’ to share this data, to ensure that learning is captured to help any further localised outbreaks.

Source: Anna Schvetz
It can help us plan better
It is important to understand the lessons learnt by governments in this pandemic, as it will help future governments to understand how to plan and react in the midst of another viral pandemic. In a similar situation, data will allow governments to interpret when to begin social distancing, how long lockdowns should last for, and what presents certain risk factors.
However, data also allows us to plan for long-term challenges as well. As countries worldwide closed schools and offices, various governments made ‘lockdowns’ a key part of their national strategy. It is important that everyone plays their role – to keep themselves and loved ones safe – but what happens when home is more dangerous than the outside world?
Shocking statistics across the globe revealed that domestic violence has surged since lockdown. The UK’s largest domestic abuse charity, Refuge, has reported a 700% increase in calls to its helpline in a single day, while cases went up by 32% in one week, in Paris by 36%, Secretary of State for Gender Equality Marlène Schiappa said.
This pressure will not end when lockdown is lifted. Not only will this have a cost on long term mental health, but also on wider society. Additionally, violence is an important issue facing communities following disasters and states will have to prepare and ensure services can cope with a rise in intimate partner violence (such as an increase in refuges, counselling services etc).
It can be difficult to predict and plan for long-term effects on anecdotal evidence alone. By putting segregated data under a lens, governments will be able to interpret regions or communities that have been adversely affected. This is not only important for domestic abuse services, but for a number of vulnerable groups that may not become immediately apparent. Only by doing this, national and local authorities can plan better services and understand where pressures might lie when life returns to normal.

Thank you for sharing. Hopefully things return to normal now.
LikeLike
Reblogged this on The Femme Fatale Collective.
LikeLike